BMI measurement and intervention in general practice
A worked PDSA cycle for improving BMI recording and weight management in your practice, fixing the data quality problems that block clinical audit, and meeting CPD requirements as a whole practice team.
Contents
A completed PDSA generates up to 9 hours of CPD across EA, RP and MO categories, applicable to all GPs in the practice. Submitted as a practice-based or group activity, one GP can record the activity for the team.
Structured team quality improvement activities contribute to a positive practice culture and are associated with GP and staff retention. The CPD gets done within practice time on problems relevant to clinical work.
Systematic BMI recording and intervention identifies at-risk patients earlier and supports better chronic disease management outcomes. A documented PDSA is ready-made evidence for RACGP accreditation.
Identifying obesity and comorbidities opens pathways for GP Chronic Condition Management Plans, Team Care Arrangements and relevant MBS items, and improves the practice data asset for PHN reporting.
BMI measurement in general practice
Approximately two in three Australian adults are overweight or obese. In general practice this proportion is higher among patients presenting with chronic conditions. Body mass index remains the recommended, practical, office-based screening tool for identifying overweight and monitoring change over time. Yet recording rates in many practices remain below PHN benchmarks, and data extraction is frequently compromised by inconsistent data entry.
A practice-wide PDSA on BMI recording addresses both the clinical gap and the data quality problem at the same time.
- Approximately 66% of Australian adults were living with overweight or obesity in 2022 (ABS National Health Survey 2022).
- Obesity is independently associated with type 2 diabetes, cardiovascular disease, obstructive sleep apnoea, certain cancers and musculoskeletal conditions.
- BMI is the recommended population-level screening tool in Australian general practice (RACGP guidelines for preventive activities in general practice).
- Data entry errors in height and weight fields are common and can prevent meaningful clinical audit and data extraction.
Why BMI recording is suited to a PDSA approach
BMI recording is measurable, auditable and directly actionable. Clinical software systems support extraction of height, weight and BMI fields. A short measurement period of one week generates meaningful data without disrupting practice flow. The tally sheet method requires no additional software configuration and scales to any practice size. Findings from each measurement week can be discussed at a brief team meeting and acted on before the next cycle.
The clinical and operational case
Identifying a patient as obese is the precondition for offering evidence-based intervention. Without a recorded BMI, the opportunity to initiate a GP Chronic Condition Management Plan or refer to allied health is frequently missed. Practices with consistent BMI recording are better positioned to identify chronic disease management pathways and to support PHN benchmarking, accreditation and population health reporting.
A secondary benefit is data integrity. Height and weight data corrupted by entry errors cannot support downstream reporting or recall. A PDSA that improves recording also improves the practice data asset.
Up to 9 hours when submitted as a practice-based or group activity: 3 EA (review of weight management evidence, clinical guidelines and the practice knowledge base), 3 RP (reviewing BMI recording rates against PHN benchmarks and setting improvement targets), 3 MO (tracking BMI capture rates, weight management discussions and review scheduling across quarterly measurement weeks). The RACGP classifies PDSA activities under Measuring Outcomes.
CPD hours from this PDSA
| Category | Focus | Hours |
|---|---|---|
| Educational Activities (EA) | Review of weight management evidence, clinical guidelines, and practice knowledge base | 3 |
| Reviewing Performance (RP) | Reviewing practice BMI recording rates against PHN benchmarks and setting improvement targets | 3 |
| Measuring Outcomes (MO) | Tracking BMI capture rates, weight management discussions and review scheduling across quarterly measurement weeks | 3 |
| Total | 9 |
GPs must complete 50 hours of CPD annually under the Medical Board of Australia registration standard. This includes at least 12.5 hours of Educational Activities, a minimum of 25 hours combined Reviewing Performance and Measuring Outcomes with at least 5 hours each, and the remaining 15 hours allocated to either as suits scope of practice. The RACGP classifies PDSA activities under Measuring Outcomes. This PDSA may be submitted as a group or practice-based activity.
How this guide works
Grey boxes with a red left border are worked examples drawn directly from Dr Chris Mitchell’s practice. They describe what the practice did, what was measured and what was learned. Off-white boxes with a dashed red border are insert boxes for your own practice. Fill these in as you complete each stage. They become the basis for your CPD submission.
Important notes
- Pharmaceutical Benefits Scheme (PBS) criteria and Medicare Benefits Schedule (MBS) item descriptors change periodically. Verify current PBS listings and MBS items against Commonwealth government sources before applying them in practice.
- Clinical content in this guide is intended as educational background only. It does not constitute clinical advice and should not substitute for clinical judgement applied to individual patients.
- Medius Global provides this guide as a professional development resource for GP practice teams. Medius Global is not a registered training organisation and does not provide accreditation services.
The PDSA cycle
Idea
The PDSA starts with a specific gap identified in the practice. For BMI recording, the trigger is typically a data audit showing recording rates below PHN peers, or a team observation that height and weight fields are inconsistently completed.
When we reviewed our BMI recording rates against PHN peers in April 2025, our rates were consistently below benchmark. We decided to focus on two things: improving the completeness of BMI recording for adult patients and ensuring that data entry was accurate enough to support meaningful extraction. We set a primary focus on patients with BMI above 35, with priority intervention for those with BMI above 40.
What gap or opportunity is driving your PDSA?
| Current BMI recording rate (if known) | |
| PHN benchmark or comparison rate (if known) | |
| Agreed focus population (for example all adults, patients with BMI above 35, chronic disease patients) |
Plan
The planning stage defines what will be measured, who is responsible and how data will be collected. Agreeing on measurement tools, measurement periods and data entry standards before the Do stage prevents avoidable errors.
We held practice meetings on 10 April 2025 and 11 September 2025 with GPs and nurses. Agreements reached:
- Each doctor records for one week per quarter using a paper tally sheet.
- Three metrics tracked each week: BMIs recorded, weight management discussions held, weight reviews scheduled.
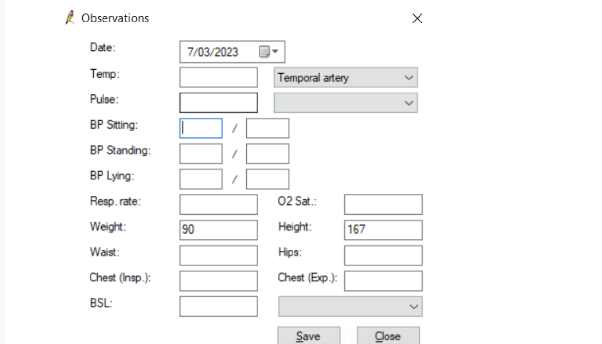
- Data entry standards: enter figures only, no units (kg or cm) in data fields, keep height and weight fields separate.
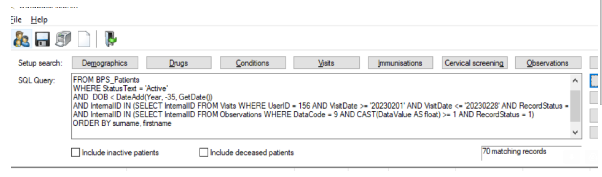
- Run active-patient searches only, exclude inactive and deceased patients.
- Submit tally sheet results every two weeks for collation.
- Intervene for all patients with BMI above 35; priority follow-up for BMI above 40.
| Planning meeting date | |
| Attendees | |
| Metric 1 to track | |
| Metric 2 to track | |
| Metric 3 to track | |
| Measurement period | |
| Agreed data entry standards |
Aims
Measurable objectives for this PDSA cycle:
- Increase the proportion of active adult patients with a recorded BMI across the measurement weeks.
- Increase the rate of documented weight management discussions for patients with BMI above 35.
- Increase the rate of weight reviews scheduled for patients with BMI above 40.
- Improve data entry accuracy in height and weight fields to enable reliable clinical software extraction.
Do: implementing the plan
The Do stage involves running measurement weeks as planned, recording on tally sheets in real time and noting any unexpected events or barriers as they occur.
We ran measurements weekly and over a quarter. Each GP recorded on a paper tally sheet during consultations. The sheet tracked BMI, recorded weight-management advice given, and scheduled weight reviews. Unexpected events during the Do stage:
- Scales were not conveniently located during consultations. We moved them to a more accessible position, which improved recording compliance.
- Data entry errors were identified early: some records showed height entered in the weight field, preventing extraction.
- Initial data searches included inactive and deceased patients, inflating denominators until corrected.
| Activity | Date |
|---|---|
| Planning meeting 1 | 10 April 2025 |
| Planning meeting 2 | 11 September 2025 |
| Measurement week 1 | April / May 2025 |
| Measurement week 2 | July 2025 |
| Measurement week 3 | October 2025 |
| Planning meeting | |
| Measurement week 1 | |
| Measurement week 2 | |
| Measurement week 3 | |
| Unexpected events during implementation |
Study: what to monitor
The Study stage compiles tally sheet results, reviews data quality findings and identifies patterns across measurement weeks.
Complete the tracking table for each measurement week:
| Metric | Week 1 | Week 2 | Week 3 | Total / trend |
|---|---|---|---|---|
| BMIs recorded | ||||
| Weight management discussions | ||||
| Weight reviews scheduled | ||||
| Data entry errors identified |
Results were recorded from tally sheets across each measurement week. We tracked BMIs recorded, weight-management advice given, and reviews scheduled. Our key data quality finding was that we were unable to extract reliable BMI data from our clinical software due to incorrect data entry. Specific issues identified:
- Height recorded in the weight field. This prevents any data search or extraction for BMI.
- Units typed into data fields alongside the auto-populated unit (for example weight showing "76kgkg" where "kg" had been typed in addition to the system value). This corrupts extraction and prevents data searches.
- Initial searches run against all patients including inactive and deceased, inflating denominators until corrected.
Our tally sheet data was collected manually and was unaffected by these extraction issues. However, any attempt to audit BMI recording via software reports produced unreliable results until data entry practices were corrected. All three data quality issues are correctable through team education and protocol changes. No software modifications are required.
Complete the tracking table above for each measurement week.
| Patterns observed across the three weeks | |
| Data quality issues identified in your clinical software | |
| What surprised you |
Data entry accuracy is a prerequisite for any meaningful BMI audit. The tally sheet method gives reliable practice-level data regardless of software extraction quality, but fixing data entry issues is necessary for any longer-term audit or PHN reporting. Moving the scales to a more accessible location in the consultation room made a practical difference to recording rates. Tally sheets were effective. They identified patients who needed BMI recorded and served as a prompt to intervene during the consultation. With a large patient database, shifting overall recording averages takes longer than anticipated. Sustained quarterly effort produces results; a single push does not. Structuring a shared practice approach to weight management was valuable in itself, independent of the data outcomes.
| What worked well | |
| What was harder than expected | |
| What you will do differently next cycle |
Act: what to change and embed
- Quarterly BMI recording weeks are now part of the practice calendar.
- Patients with BMI above 40 are flagged for priority follow-up.
- Data entry standards embedded in team protocols: figures only, no units in data fields, keep height and weight fields separate.
- Active-patient-only filtering is the standard for all practice data searches.
- Team learnings are shared at a brief post-week meeting before each new quarterly cycle.
| Change 1 you are embedding | |
| Change 2 you are embedding | |
| Change 3 you are embedding | |
| Next measurement week date | |
| Next PDSA topic under consideration |
Submitting for CPD hours
Submit this PDSA via the RACGP CPD portal at portal.racgp.org.au/CPD. Select GP-led activity (individual or group) and PDSA as the activity type.
Submit as a group or practice-based activity via the RACGP portal for each of the participating GPs, consider the time committed to each cycle, but submit collated times, averaged across each GP to reduce the administrative burden.
Doctors involved
Record the GPs who participated in this PDSA.
| Doctor’s name | CPD number |
|---|---|
Resources
- RACGP HANDI: Ten Top Tips for weight control
- RACGP guidelines for preventive activities in general practice (the red book)
- Therapeutic Guidelines: Endocrinology
- NSW Government Get Healthy program (free telephone health coaching)
- Active and Healthy NSW (find local exercise programs)
- Healthdirect service finder (locate dietitians and exercise physiologists by area)
- My Community Directory (community services and social prescribing)
Running a PDSA in your practice?
Medius Global supports GP practice owners and managers across practice assessment, compliance, operations and business development. If your practice is working through quality improvement, accreditation preparation or transition planning, we can help.
Contact us: mediusglobal.com.au
Background and reference
This section forms part of the Educational Activities (EA) component of your CPD submission. Read it before or alongside the PDSA cycle to build the knowledge base for your weight management interventions.
Weight management in general practice
Obesity is a serious, chronic and progressive condition associated with significantly increased all-cause mortality and a range of comorbidities: type 2 diabetes mellitus, hypertension, dyslipidaemia, coronary heart disease, obstructive sleep apnoea, certain cancers, urinary incontinence and depression.
The benefits of weight loss include reduced progression from impaired glucose tolerance to type 2 diabetes, reduced blood pressure in hypertensive patients, improved lipid profiles and improvements in quality of life, physical functioning and mobility.
Initial management approach
The initial management for patients who would benefit from weight loss is a structured lifestyle intervention combining dietary modification, increased physical activity and behavioural support. Treatment selection is based on initial risk assessment.
- All patients who would benefit from weight loss should receive counselling on diet, exercise and realistic goals.
- Pharmacologic therapy candidates: adults with BMI 30 kg/m² or above, or BMI 27 to 29.9 kg/m² with comorbidities, who have not achieved at least 5% weight loss at three to six months with a structured lifestyle intervention.
- Bariatric surgery candidates: adults with BMI 40 kg/m² or above, or BMI 35 to 39.9 kg/m² with at least one serious comorbidity, who have not met weight loss goals with diet, exercise and pharmacotherapy.
Dietary approaches
No single diet has demonstrated sustained superiority for weight loss. Any approach that achieves sustained caloric restriction will produce weight loss. The Mediterranean diet is the only dietary pattern with demonstrated benefit on hard clinical outcomes including mortality, independent of weight change.
Intermittent fasting and continuous caloric restriction produce similar weight loss at six to twelve months (approximately 5 to 9 kg). Ketogenic diets produce approximately 2 kg more weight loss than low-fat diets at one year in higher-quality studies, with no sustained difference beyond that. Discontinuation rates with all approaches reach approximately 60% at one year.
Practical advice for patients:
- Target realistic weight loss of 1 kg per month.
- A portion-controlled Mediterranean diet is supported by most clinical authorities.
- Extending the fasting window and reducing liquid calories (water as the default drink) are practical starting points.
- Self-monitoring calorie intake using a tracking application (for example MyFitnessPal) helps motivated patients.
- Very low calorie diet programs (for example Optifast) are evidence-supported options for patients requiring structured intervention.
- Refer to a dietitian for assessment and ongoing support.
Physical activity
Physical activity is less potent than dietary restriction for weight loss but is a strong predictor of weight loss maintenance and reduces loss of lean muscle mass during active weight loss. Recommended baseline: at least 30 minutes of moderate activity, five to seven days a week, to prevent weight gain. Significantly greater volumes are needed to produce weight loss in the absence of dietary restriction.
A multicomponent program including aerobic and resistance training is preferred. Exercise prescription should account for existing medical conditions, age and patient preferences. Refer to an exercise physiologist for patients with complex needs or significant comorbidities.
Medication review
Before initiating pharmacotherapy, identify medications that may cause or contribute to weight gain and switch to weight-neutral or weight-reducing alternatives where clinically appropriate.
- Diabetes management: insulin, sulfonylureas, thiazolidinediones and meglitinides cause weight gain; GLP-1 agonists, SGLT-2 inhibitors and metformin are weight-neutral to weight-reducing.
- Migraine prophylaxis: propranolol causes weight gain; topiramate is weight-reducing. Topiramate is teratogenic; use with appropriate caution in women of childbearing age.
- Antidepressants and antipsychotics: review for weight impact when initiating or reviewing.
Weight management pharmacotherapy
GLP-1 receptor agonists
GLP-1 receptor agonists are the recommended first-line pharmacotherapy for obesity where lifestyle intervention has not achieved target weight loss.
Semaglutide (Ozempic / Wegovy)
- Ozempic (semaglutide for type 2 diabetes): PBS-listed for type 2 diabetes. Starting dose 0.25 mg weekly for 4 weeks; increase to 0.5 mg, then up to 2 mg per product information.
- Wegovy (semaglutide 2.4 mg for weight management): as at June 2026, not PBS-listed for general weight management. In November 2025 the PBAC recommended a narrow listing for adults with established cardiovascular disease and obesity, limited to BMI 35 kg/m² or above (32.5 kg/m² or above for patients of Asian, Aboriginal or Torres Strait Islander background). As at June 2026 the listing process has not completed and Wegovy is not PBS-listed for any indication. It remains available on private prescription. Verify current status against the Schedule of Pharmaceutical Benefits before prescribing.
Efficacy: used with lifestyle modification, semaglutide 2.4 mg weekly produces approximately 10 to 15% body weight reduction at 68 weeks versus 2 to 3% with placebo. Approximately 70 to 80% of patients achieve 5% or more body weight loss.
Side effects: gastrointestinal effects (nausea, vomiting) are common. Weight regains after cessation.
Monitoring: gallbladder disease, acute pancreatitis symptoms. An association with non-arteritic anterior ischaemic optic neuropathy (NAION) has been reported; exercise caution in patients with existing risk factors for this condition.
Tirzepatide (Mounjaro)
- TGA-approved for type 2 diabetes. As at June 2026, not PBS-listed for any indication in Australia. In April 2026 Eli Lilly declined the PBS listing conditions offered. Available on private prescription only.
- SURMOUNT-1 data: approximately 20 to 22% body weight reduction with tirzepatide, compared with approximately 15% for semaglutide. Individual responses vary significantly.
- Starting dose 2.5 mg weekly; increase by 2.5 mg increments at minimum 4-week intervals. Maintenance doses: 5 mg, 10 mg, 15 mg weekly.
- Side effects and monitoring considerations similar to semaglutide.
Other pharmacotherapy
- Orlistat (Xenical): modest proven benefit on glycaemia, lipids and blood pressure. Frequently not tolerated due to gastrointestinal side effects. Not first-line given the established profile of GLP-1 agonists.
- Phentermine (Duromine): approved for short-term use (12 weeks) only. Higher side effect profile and abuse potential. Lowest cost option; some clinicians use for extended periods based on clinical experience.
- Combination bupropion-naltrexone: similar weight loss to orlistat; more contraindications. Cardiovascular risk uncertainty limits use. Monitor for neuropsychiatric side effects.
After initiating any pharmacotherapy: review weight loss, blood pressure and heart rate at six weeks. If less than 4 to 5% body weight reduction at 12 weeks at maximum tolerated dose, taper and discontinue.
Bariatric surgery
Bariatric surgery produces the greatest and most sustained weight loss. Eligibility: BMI 40 kg/m² or above, or 35 kg/m² or above with at least one serious comorbidity, where diet, exercise and pharmacotherapy have not achieved target weight loss.
Roux-en-Y gastric bypass (RYGB): approximately 22% net body weight reduction at one year. Laparoscopic sleeve gastrectomy: approximately 15% net body weight reduction. Both approaches produce significant improvement in type 2 diabetes, hypertension and dyslipidaemia. Refer to a bariatric surgeon for pre-surgical assessment.
Annual CPD requirements
| Category | Minimum annual hours | Notes |
|---|---|---|
| Educational Activities (EA) | 12.5 | Reading, online learning, structured education, knowledge base review |
| Reviewing Performance (RP) | 5 minimum | Part of combined RP and MO minimum of 25 hours |
| Measuring Outcomes (MO) | 5 minimum | RACGP classifies PDSA under MO |
| Total annual requirement | 50 | Remaining RP and MO hours allocated as suits scope of practice |