Managing a practice is not the same as running one
Most GP practice owners see their practice manager as the person who keeps operations running smoothly; appointments flow, staff are rostered, correspondence is managed, and filing is completed. This describes a valuable practice administrator, but the role is distinct from that of a business manager.
A practice manager, in how the role has historically operated across Australian general practice, is focused on operational management. They manage what is in front of them. A business manager oversees the financial strategy, drives income growth, manages risk across multiple domains, and makes decisions that determine where the practice is heading, not just whether it opens on time tomorrow.
The Business Manager is a critical member of your practice's professional advisory team: Accountant, Lawyer, Financial advisor and Business manager.
GP practice owners are, almost without exception, clinicians who ended up running a business. Many understand that strong management is necessary, but have no clear framework for what that looks like in practice, what they should be asking for, or what a capability gap costs them over time.
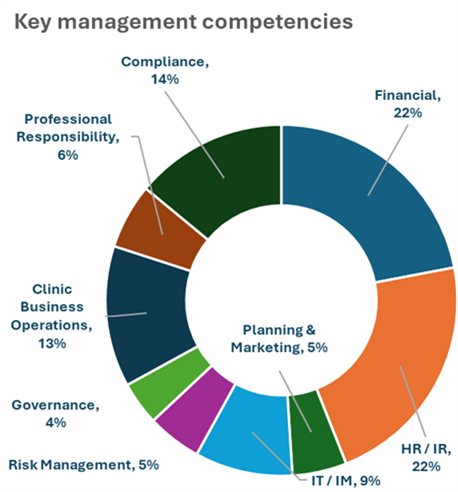
The nine competency areas below define the full scope of the role. These areas outline where the strongest pressures fall and provide practice owners with tangible criteria for hiring, evaluating, or restructuring management, making clear what standards to expect from a business manager.
The nine key competency areas of a business manager
GP practice management covers nine domains, each with technical and regulatory requirements. The percentages below represent how my framework weights management responsibilities across these areas, based on experience in various practice environments.
No practice manager excels equally in all nine domains. Business managers differ in their ability to keep all domains in view, act decisively in high-risk areas, and judge when to seek specialist input.
Where the pressure concentrates
Financial management and HR/industrial relations each sit at 22% of the framework. These two areas produce the highest risk and the costliest remediation when poorly managed. IT and information management, at 9%, is a growing third pressure point as practices navigate My Health Record obligations, My Medicare registration, electronic prescribing, practice software environments and an expanding set of data security requirements.
Strong management in these three areas (financial, HR and IT) leads to measurable differences in financial results, compliance status, and overall practice value. Prioritising expertise here is critical for success and long-term sustainability.
1. Financial management (22%)
A business manager with comprehensive financial competency covers the full span of what the role requires: developing a financial strategy that reflects the practice's business plan, managing income across multiple streams, controlling and reducing expenses, running payroll accurately, managing the budget and producing financial reporting that informs management decisions rather than just satisfying legislative obligations. The distinction between management reporting and accountancy reporting is one that many practices have never made clearly. A capable business manager makes it as a matter of course.
The federal government's focus on bulk billing across much of the sector has changed the economics of general practice, making this function more demanding than it was five years ago. Mixed billing models require active management of fee structures, billing compliance and gap payment processes. Practices that were financially well-managed under a predominantly bulk-billing model are now finding that the same level of oversight is insufficient. The margin for error is narrower, and the cost of poor financial visibility is higher.
Income development is where this competency gets the least attention in most practices. A business manager working at the right level asks whether the current service mix is appropriate, whether the practice is not capturing revenue streams, and whether the fee schedule reflects the actual cost of delivering care. These are financial management questions within the practice manager's remit.
The compliance dimension of financial management has also sharpened. Two key areas involving governance are dominating the general practice landscape:
i. The emergence of My Medicare (patient registration) and the link to allowable MBS item payments may be construed as a move to a nationalised system determined to reduce opportunistic payment of higher value items.
ii. Payroll tax exposure for contractor GPs has become a material issue across multiple states following a series of court decisions, and practices that have not reviewed their contractor arrangements against current case law and relevant State Revenue Office guidance are carrying undisclosed liability.
The key takeaway is that a business manager with strong financial and compliance grounding should raise concerns with the practice owner and ensure specialist advice is sought.
2. Human resources and industrial relations (22%)
HR and IR carry the same 22% weighting as financial management in the framework. In terms of acute operational disruption, it may be the sharper of the two risks. Financial problems tend to build gradually. HR problems surface fast and, if handled badly, become expensive quickly.
General practice employs a complex staff mix. Reception and administrative staff sit under the Health Professionals and Support Services Award (MA 000027). Nurses sit under the Nurses Award (MA 000034). GPs and other practitioners may be employees, contractors or associates, depending on the practice model, and the distinctions carry significant legal and financial consequences. The contractor-versus-employee question is not a matter of what the contract says. It is a matter of what the working relationship looks like in practice, and the case law on this has moved against practices that have not recently reviewed their arrangements.
The Fair Work Act, the National Employment Standards, relevant awards, WorkSafe obligations and state legislation all apply, often simultaneously. A business manager does not need to be an employment lawyer. They need to know enough to manage employment relationships correctly day to day, to keep documentation in order, and to recognise when a situation requires specialist advice.
Most practice HR problems are not complex legal questions. They are failures of basic processes: position descriptions that do not reflect actual roles, performance appraisals that never happened, rosters set without reference to award minimums, hiring done without appropriate contracts in place, or terminations handled informally, leaving the practice exposed. These are preventable. They become expensive when a business manager either lacks the knowledge to manage them correctly or lacks the authority to implement appropriate processes.
Wages, rosters, hours, training, coverage, and formal review are all HR functions that require active, informed management. So is the hiring and firing process, including the contract and position description work that underpins it. A capable business manager also creates a practice culture where staff understand what is expected, feel appropriately supported and want to stay. In a sector where COVID had a significant negative impact, finding good clinical support staff is not easy, and the cost of turnover is substantial; this is not a secondary consideration.
3. Compliance (14%)
Compliance in general practice is not a single regulatory obligation. It is a continuous operational requirement across multiple frameworks, each with its own audit appetite and its own consequences for non-compliance.
The relevant bodies and frameworks include Medicare, private health insurers, the ATO (PAYG, Superannuation Guarantee Levy and BAS), ASIC, AHPRA, WorkSafe, and State Revenue Office obligations, including payroll tax. Federal, state and local government legislation all apply. Planning and parking requirements, local compliance items and the obligations that flow from being a registered health service are also part of this picture.
A business manager with genuine compliance competency does more than complete an accreditation checklist every three years. They maintain a working knowledge of the practice's obligations, consistently monitor regulatory changes, and ensure operational systems are always ready. Top-performing practices treat accreditation as a confirmation of their usual operations, not an intensive catch-up process.
4. Clinic business operations (13%)
This competency covers the operational backbone of daily practice: appointment management, patient flow, clinical rosters, billing workflows, after-hours arrangements, policies and procedures, and the processes that determine whether a practice runs well.
What distinguishes a business manager in this area is not whether they can manage these functions but whether they actively improve them. The questions they ask are different: Is the service mix right for this patient cohort? Is there a competitive edge the practice could develop, or is it already developing but not being clearly positioned? Are clinic hours structured around service delivery, cost and sustainable clinical workload, or have they accumulated by default? Are systems and process efficiencies being applied to reduce repetition, through secure messaging for letters, online appointments and electronic results?
An observation worth emphasising: in some practices, the business manager or the principal GP is the competitive edge. The reputation, the relationships, the clinical capability or the management approach that makes the practice preferable to patients and practitioners. Recognising and articulating that is part of the strategic function, and it matters for GP recruitment, patient growth and, eventually, practice value.
5. IT and information management (9%)
IT carries 8% of the competency framework weighting, which understates its operational criticality. The consequences of IT failure in a GP practice are not theoretical. Software failure stops consulting. A data breach is a Privacy Act matter. A poorly managed upgrade disrupts billing and patient records.
The requirements in this area include software and hardware maintenance across the practice management system, managing implementation and upgrades, including online appointments, cloud computing, clinic apps and wi-fi check-in, eHealth obligations, including My Health Record and My Medicare, data security and off-site back-up with confirmed restore capability, website maintenance, and navigating the adoption of AI and emerging technology within the practice.
A business manager does not need to be a technologist. They need to be technically literate enough to manage vendor relationships, identify when a problem exceeds internal capability, ensure the practice's technology environment meets its obligations under the Privacy Act and health privacy legislation, and train staff to use the systems well rather than around them.
IT is increasingly a due diligence item in practice sales. A practice with a well-maintained software environment, clean data and documented security processes presents differently from one where IT has been managed reactively. The business manager who has kept this in order has directly protected practice value.
6. Professional responsibility (6%)
Professional responsibility covers the business manager's own development and its direct effect on practice culture.
For the business manager, this includes maintaining their knowledge base through continuing professional development, sustaining membership of relevant professional associations, and keeping up with the regulatory changes that affect the practice through IR update services, Medicare update reminders and relevant LinkedIn specialist groups.
The culture dimension carries more operational weight than a 6% weighting might suggest. A business manager who is professionally engaged and visibly committed to their own development sets a standard that the rest of the practice team notices. Culture in a GP practice is not a mission statement on a wall. It is the aggregate of how the team operates, how problems are handled, how patients are treated, and what standards are consistently upheld. In most practices, the business manager is the primary driver of that culture.
7. Risk management (5%)
Risk management in a GP practice covers clinical incident risk, which intersects with professional responsibility and AHPRA obligations, OH&S compliance, business continuity, technology risk, and financial risks arising from poor billing practices, inadequate insurance, or weak contract management.
A business manager with sound risk management practices works with the practice's medical defence organisation and insurers, maintains current, specifically followed policy and procedure manuals, ensures induction and training processes reduce preventable incidents, and keeps the physical environment compliant with OH&S requirements. Some practices have found value in having the local police conduct a security review of the premises, which is an underused and straightforward measure.
Business continuity is where most practices are most underprepared. What happens if the practice management software is unavailable? If the principal GP is incapacitated? If a key staff member leaves with no notice? If there is a data breach? A capable business manager has worked through these scenarios, has documented responses for the most likely ones, and has ensured the practice is not dependent on a single point of failure in its daily operations.
8. Planning and marketing (5%)
Planning in a GP practice is not corporate strategic planning. It is the practical discipline of setting objectives for the practice and tracking performance against them, informed by data and structured around a genuine business plan.
The PDSA cycle (Plan, Do, Study, Act) is a useful operational planning tool in practice, particularly for quality improvement and project-based work. The planning function also includes maintaining a clear view of the patient cohort, understanding the practitioner mix and its implications for income and service delivery, knowing the local competitive environment well enough to identify gaps and opportunities, and supporting the practice owner in capital and expansion decisions.
Marketing for a GP practice has both internal and external dimensions. Internally, it covers how the practice presents to patients and referring practitioners: the letterhead, waiting room materials, the patient newsletter, the footer on correspondence that highlights secure messaging capability, and the educational content that builds the practice's standing in the local clinical community. Externally, it covers the website, social media strategy, SEO, video content and digital presence. Educational sessions for referring practitioners and consulting sessions at external specialist rooms are also marketing activities with a relationship-building function.
Advertising for medical practices in Australia is heavily regulated, and a manager needs to be aware of those regulations; AHPRA publishes the regulatory guidelines: Medical Board of Australia: Guidelines for advertising a regulated health service.
Knowing the patient cohort, understanding what referring practitioners value, and building relationships with hospitals and third-party contract providers are all planning and marketing activities that a business manager at the right level will be actively managing.
9. Governance (4%)
Governance sits at 4% of the framework weighting, but its absence tends to surface at the worst possible moments: an AHPRA inquiry, a Medicare audit, a staff dispute, or a due diligence process for a practice sale.
Governance means established policies and procedures that the practice adheres to, a Code of Ethics aligned with the relevant professional bodies (AMA, RACGP, AAPM), a functioning management structure across legal, financial and administrative matters, a staff charter and a patient charter, and documentation practices that demonstrate the practice operates with appropriate accountability.
A governance-minded business manager does not treat policies and procedures as accreditation documents. They treat them as the practice's operating standards, reviewed and updated as the practice changes, and understood by all staff.
Peter Drucker put the distinction plainly: 'Management is doing things right; leadership is doing the right things.' A practice can be operationally competent and still be heading in the wrong direction. Governance, culture and strategic oversight are the functions that keep those two things aligned.
The litmus test
Ask yourself: is the person who manages your practice someone you would trust to have a full, unfiltered conversation about your financial performance, compliance exposure, HR obligations, and the practice's strategic direction? Not a summary of what is going well, but an honest assessment that includes the gaps, the risks and the decisions that need to be made.
If the answer is yes, you have a business manager. If the answer is 'mostly', 'not really' or 'I've never tried', the role is not operating at the level the practice needs.
The practices that perform well under external scrutiny:
- exhibit sustainability,
- achieve profitability,
- maintain their compliance standing,
- achieve strong accreditation outcomes and
- present well at due diligence
Those practices are, with very few exceptions, those in which the management function is operating at the optimal level.
The nine competency areas above are not a job advertisement checklist. They are a diagnostic. Used pragmatically, they show a practice owner where management is strong, where it is adequate and where the gaps are carrying real risk.